File:Methods of imaging the lymphatic system.jpg
Jump to navigation
Jump to search

Size of this preview: 415 × 599 pixels. Other resolutions: 166 × 240 pixels | 332 × 480 pixels | 532 × 768 pixels | 709 × 1,024 pixels | 2,250 × 3,250 pixels.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Original file (2,250 × 3,250 pixels, file size: 754 KB, MIME type: image/jpeg)
Captions
Captions
Methods of imaging the lymphatic system.
Summary
[edit]{kind=link}
| Description |
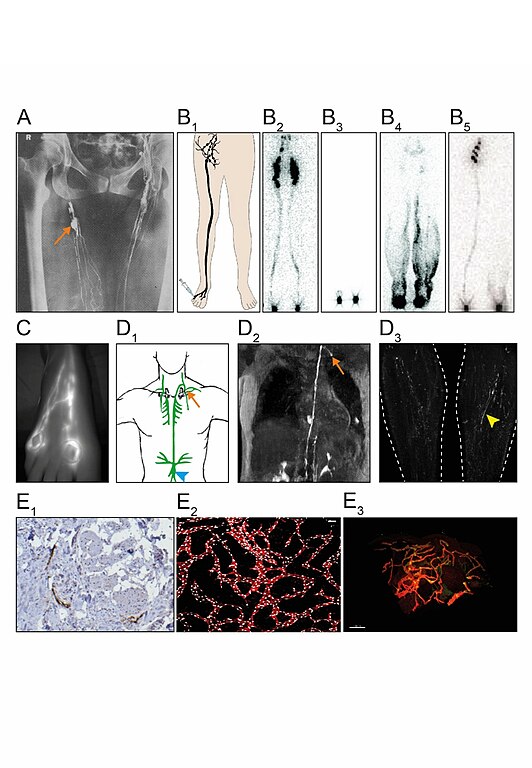
English: (A) Direct contrast X-ray lymphography involves the injection of an x-ray contrast agent e.g. Lipiodol. First, lymphatic vessels are identified by subcutaneous injection of a vital dye e.g. patent blue. Under local anesthetic, an incision is then made to expose the lymphatic vessel following the insertion of a needle into its lumen. The contrast agent can then be injected, and radiographs taken. Clear definition of lymphatic collectors and lymph nodes (arrow) can be achieved, but the procedure is invasive and rarely performed. (B1) Lymphoscintigraphy involves the injection of Technetium-99 into the web spaces between the toes (or fingers). Images using a gamma camera can be taken at specified time intervals and reveal lymph drainage channels with uptake of the contrast agent in regional lymph nodes. Removal of the contrast agent from the injection site and uptake in nodes reflect lymph transport (quantitative lymphoscintigraphy). (B2) Anterior view of a normal subject. (B3) Milroy patient carrying a VEGFR3 mutation showing no uptake by the initial lymphatics nor transport to the lymph nodes (functional aplasia). (B4) Lymphedema distichiasis syndrome patient carrying a FOXC2 mutation showing lymph reflux with dermal backflow seen as dark shading in the calf. (B5) Emberger patient carrying a GATA2 mutation exhibiting unilateral uptake, with the left leg showing no migration of tracer within the collecting lymphatics. (C) Indocyanine Green lymphography (ICGL) imaging of the right dorsal foot. Two indocyanine green intradermal injections are given in the toe web spaces followed by an immediate absorption of ICG into initial lymphatics. Excitation of the area of interest with laser or LED will emit fluorescence through the skin, that allows for real-time imaging with a near-infrared detector camera to visualize lymph drainage up the leg. Contractility of lymphatic collectors can be seen in real time. (D1+2) Dynamic contrast-enhanced magnetic resonance lymphangiogram (DCMRL) can image lymphatic vessels. Following bilateral injection of contrast under ultrasound guidance directly into an inguinal lymph node, central conducting vessels can be seen, like the cisterna chyli (arrowhead) and thoracic duct, highlighted in green in the drawing of the upper chest. The image is a T1 weighted MRI in which areas of contrast uptake appear bright demonstrating the thoracic duct terminating at the junction of the left subclavian and internal jugular veins, into which it drains (arrow). (D3) T2 weighted images demonstrate high signal in areas of static or slow-moving fluid. Vessel-like structures can be observed bilaterally in the legs (arrowhead). Whether these structures represent lymphatic or venous vessels remain controversial. Imaging of skin biopsies has advanced considerably with the development of modern microscopy techniques and the use of antibodies against lymphatic-specific markers. (E1) Immunohistochemistry (IHC) on paraffin-embedded 2D human skin sections showing podoplanin (PDPN) positive lymphatic vessels (brown DAB staining). Image taken at 20X magnification with a light microscope. (E2) Dermal lymphatic vasculature in the developing mouse embryo. Skin whole-mount preparation of E14.5 wildtype mouse embryos are visualized in 3D using a confocal microscope. Lymphatic endothelial cells are identified by Prox1 (white) and Vegfr3 (red) expression. Maximum intensity projections are shown. Scale bar = 100 µm. (E3). Whole-mount 3D human skin biopsy from a healthy control optically sectioned using a light sheet microscope and VIPAR analysis (164). Lymphatic endothelial cells are identified by PROX1 (green) and PDPN (red) expression. Scale bar = 100 µm. |
| Date | |
| Source | Own work |
| Author | SGUL lymres |
Dr Malou van Zanten, St. George’s University of London; Dr Lakshmi Ratnam, St. Georges Hospital NHS Trust, London; Dr Rene Hägerling, Charité, Berlin; Sif Nielsen and eLearning Unit members Sheetal Kavia and Dhillon Khetani from St George’s, University of London (SGUL) have assisted with figure preparation.
Licensing
[edit]{kind=link}
I, the copyright holder of this work, hereby publish it under the following license:
This file is licensed under the Creative Commons Attribution-Share Alike 4.0 International license.
- You are free:
- to share – to copy, distribute and transmit the work
- to remix – to adapt the work
- Under the following conditions:
- attribution – You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.
- share alike – If you remix, transform, or build upon the material, you must distribute your contributions under the same or compatible license as the original.
File history
Click on a date/time to view the file as it appeared at that time.
| Date/Time | Thumbnail | Dimensions | User | Comment | |
|---|---|---|---|---|---|
| current | 11:48, 29 January 2021 | | 2,250 × 3,250 (754 KB) | SGUL lymres (talk | contribs) | Uploaded own work with UploadWizard |
You cannot overwrite this file.
File usage on Commons
There are no pages that use this file.
File usage on other wikis
The following other wikis use this file:
- Usage on es.wikipedia.org
- Usage on it.wikipedia.org
{kind=link}